
{kind=link}
{kind=link}
放射治疗ⅠE期非结膜眼附属器黏膜相关淋巴组织型淋巴瘤的剂量效应和预后
[赵水喜1 , 俞立权1 , 布洁1 , 曹京旭1 , 肖利华2  ]
]
]
|
|


作者简介:赵水喜,硕士,副主任医师。
目的 评价放射治疗ⅠE期非结膜原发眼附属器黏膜相关淋巴组织型淋巴瘤的剂量效应和预后。方法 回顾性分析2003-11至2012-03收治的影像资料完整可测量33例(42只眼)ⅠE期非结膜原发眼附属器黏膜相关淋巴组织型淋巴瘤患者资料。结果 照射剂量18 Gy时与27 Gy时,依据WHO标准评价疗效,缓解率分别为31%和42.9%( P=0.258);依据RECIST标准评价疗效,缓解率分别为28.6和38.1%( P=0.355)。全组患者局部控制率100%。全组患者的5年、10年总生存(OS)率分别为96.8%和84.7%; 5、10年无进展生存(PFS)率分别为89.6%和89.6%。接受≥30.6Gy组与27 Gy组,5、10年总生存(OS)率分别为100%、80%和95.7%、95.7%( P=0.8578); 5、10年无进展生存(PFS)生存率分别为83.3%、83.3%和91.1%、91.1%( P=0.6497)。结论 非结膜原发眼附属器黏膜相关淋巴组织型淋巴瘤对放射治疗敏感。从局部控制和长期生存的观察结果显示,27 Gy的照射剂量是足够的。探索最佳的照射剂量需要开展前瞻性大样本的剂量效应观察研究。
Objective To evaluate the dose response of patients with ⅠE stage non-conjunctival primary ocular adnexal mucosa associated lymphoid tissue lymphoma(POAML) treated with primary radiotherapy.Methods Clinical data on thirty-three patients(42 eyes) with stage Ⅰnon-conjunctival POAML treated between November 2003 and Match 2012 were retrospectively studied.Results For all the patients, the local control rate was 100% at the dose of 18 Gy and 27 Gy, while the response rate was 31% and42.9%( P=0.258)respectively as measured with the WHO criteria. However, the response rate was 28.6% and38.1%( P=0.355)respectively as measured with the RECIST criteria. For patients of non-conjunctival POAML treated at the dose of ≥30.6 Gy and 27 Gy, the five-year overall survival(OS) rate was 100% and 95.7% respectively ( P=0.8578), and the five-year progression-free survival(PFS) rate was 83.3% and 91.1% respectively ( P=0.6497).Conclusions The prescribed dose of 27 Gy for non-conjunctival POAML seems to be effective. Prospective clinical studies should be carried out to define the optimal dose for POAML.
眼附属器淋巴瘤占全身淋巴瘤的2%[1, 2], 占全身结外病变的6%[3]。眼附属器原发淋巴瘤最常见的组织亚型为黏膜相关淋巴组织型淋巴瘤, 占眼眶原发淋巴瘤的比例西方国家为36%~66%[4, 5, 6, 7], 日韩的比例为80%~98%[8, 9, 10, 11, 12, 13]。临床实践显示单纯放疗Ⅰ E期病变可以获得良好的局部控制和长期生存[14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29]。然而目前尚无一致可接受的处方剂量推荐[14, 16, 18, 21, 22, 25, 27]。眼附属器黏膜相关组织型淋巴瘤放疗后消退缓慢[18, 22, 24, 25, 30], 一些学者试图尝试进一步补量获得肿瘤完全缓解, 结果带来严重的并发症[14, 19, 25, 30]。本研究依据WHO、RECIST疗效评价标准回顾性分析放射治疗非结膜眼附属器黏膜相关组织型淋巴瘤的剂量效应和预后。
选取2003-11至2012-03收治的影像可评价33例, Ⅰ E期非结膜原发眼附属器黏膜相关组织型淋巴瘤。男28例, 女5例。年龄33~85岁, 中位年龄59岁。原发双眼病变10例, 右眼眶10例, 左眼眶13例, 共43眼。影像可测量42眼。剂量27 Gy, 23例(29眼); 30.6~45 Gy, 10例(13眼)。
临床分期检查包括病史、体格检查; 化验检查包括血常规、肝肾功能、乳酸脱氢酶、血沉、风湿因子、蛋白电泳、免疫球蛋白(IgA、IgG、IgM、IgE)、免疫球蛋白G亚型(G1、G2、G3、G4)、白介素2、甲状腺功能全项; 眼眶MRI或CT; 胸部、腹部、盆腔CT; 骨髓活检。采用Ann Arbor分期原则, Ⅰ E期定义为原发肿瘤局限眼眶, 单侧病变或同时发生的双侧病变。
全部患者采用CT模拟定位。眼眶病变放疗临床靶体积为排除眼球的全眼眶。计划靶体积为临床靶体积外放3 mm。19只眼采用悬挂挡铅遮挡晶体, 3只眼采用接触式铅屏蔽遮挡晶体。放疗中位剂量27(27~45)Gy, 分次剂量180c Gy。23例29只眼接受27 Gy照射, 10例13只眼接受30.6~45.0 Gy照射。
分别依据WHO疗效评价标准和RECIST疗效评价标准评价近期疗效。总生存时间指放疗开始时间到死于任何疾病、最后随诊日期或截止观察日期。无进展生存是指放疗开始时间到疾病复发、进展或最后随诊日期或截止观察日期。
采用SPSS10.0软件进行数据分析与处理, 生存率分析采用Kaplan-Meier方法, 组间生存率比较采用Log-rank检验, 组间率的比较采用χ 2检验, P< 0.05为差异有统计学意义。
全组患者局部控制率100%。全组患者的5年、10年OS率分别为96.8%和84.7%; 5年、10年PFS率分别为89.6%和89.6%(图1)。
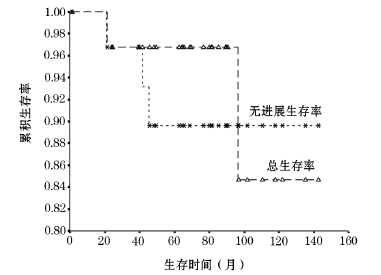 | 图1 全组总生存率和无进展生存率曲线 Ⅰ 期原发非结膜眼附属器黏膜相关淋巴组织型淋巴瘤单纯放疗全组总生存率和无进展生存率曲线(5年、10年OS率分别为96.8%和84.7%; 5年、10年PFS率分别为89.6%和89.6%) |
(1)WHO标准疗效评价: 42只眼接受≥ 27 Gy, 放疗前病变长径最大垂直径积中位471.5(80~1410)mm2, 18 Gy后病变长径最大垂直径积中位245(0~784)mm2, 27 Gy时病变长径最大垂直径积中位241.5(0~650)mm2。18 Gy时与27 Gy时病变缓解率分别为31%(13/42)和42.9%(18/42), 差异无统计学意义(P=0.258)。(2)RECIST标准疗效评价:42只眼接受≥ 27Gy, 放疗前病变长径中位26(12~44)mm, 18Gy后病变长径中位20.5(0-39)mm, 27Gy时病变长径中位20(0~39)mm。18Gy时与27Gy时病变缓解率分别为28.6(12/42)和38.1%(16/42), 差别无统计学意义(P=0.355)。
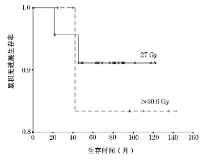
(1)放疗反应与预后: 放疗27 Gy时应用WHO评价放疗缓解与稳定者5年OS率分别为92.3%和100%(P=0.5151); 5年PFS生存率分别为91.7%和88.2%(P=0.7051)。应用RECIST评价放疗缓解与稳定者5年OS率分别为90%和100%(P=0.2588); 5年PFS率分别为88.9%和90%(P=0.9980)。(2)剂量与预后 :接受≥ 30.6 Gy组与27 Gy组, 5年、10年OS率分别为100%、80%和95.7%、95.7%(P=0.8578); 5年、10年PFS生存率分别为83.3%、83.3%和91.1%、91.1%(P=0.6497, 图2)。
 | 图2 照射剂量≥ 30.6 Gy和27 Gy的无进展生存率曲线 比较照射剂量≥ 30.6 Gy和27 Gy的无进展生存率曲线(5年、10年PFS生存率分别为83.3%、83.3%和91.1%、91.1%) |
3例治疗后失败, 失败部位为扁桃体、食管、肺部、全身多发淋巴结。3例失败时间分别为放疗后21、42、45个月。
全组3级白内障发生率27.9%(12/43)。采用晶体减免技术与晶体未遮挡者3级白内障发生率13.6%(3/22)和42.9%(9/21)(P=0.045)。
有研究显示, Ⅰ E期眼眶黏膜相关淋巴组织型淋巴瘤单纯放射治疗5年局部控制率93%~100%, 5年、10年生存率分别为84%~100%和73%~86%, 5年、10年无进展生存率分别为76%~96%和70%~93% [14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29]。本研究中, 5年、10年局部控制率均为100%, 5年、10年生存率分别为96%和84.7%; 5年、10年无进展生存率分别为89.6%和89.6%, 和文献报道相似。
眼附属器黏膜相关组织型淋巴瘤放射治疗剂量研究来自临床回顾性分析结果。Ejima等[22]报道42例患者放疗结果, 靶区最小剂量24 Gy, 5年局部控制率100%。Goda等[27]报道89例放疗结果, 照射剂量25 Gy, 7年局部控制率97%。文献[14, 18, 21, 25, 27]结果显示, 接受20 Gy以上剂量照射均获得满意的局部控制, 30 Gy、30.6 Gy、34 Gy剂量水平治疗效果无差别。本研究中, 结果显示照射剂量≥ 30.6 Gy和27 Gy者局部控制和长期生存无明显差别。然而Fung等[16]报道39例患者治疗结果显示, 照射剂量< 30 Gy和 ≥ 30 Gy局部控制率分别为81%、100% (P< 0.01)。明确最佳照射剂量, 迫切需要开展较大样本的临床剂量反应观察研究。
放射治疗结束后为一种缓慢消退的过程。Son等[25]报道放疗后4~6周评价时54%患者获得完全缓解, 中位随访32.3个月后93%患者获得完全缓解, 部分缓解病变达到完全缓解中位时间2(0.1~25)个月。Jung等[30]回顾性定量研究非结膜眼眶病变的治疗后消退规律, 定义残存病变体积无进一步的变化为达到最大肿瘤反应, 治疗后6个月内75%以上的患者达到最大肿瘤反应, 获得最大肿瘤反应中位时间6(3~18)个月。本研究回顾性分析非结膜眼眶黏膜相关组织型淋巴瘤放疗期间消退, 结果显示放疗18 Gy时肿瘤已经出现消退, 肿瘤对放射治疗敏感; 放疗18 Gy、27 Gy时消退趋势与Jung 研究结果一致。本研究结果发现, 对于缓慢消退的肿瘤, 无法判断最佳肿瘤照射剂量。Gayed等[31]应用PET评价放疗后影像残存, 结果显示残存无FDG摄取, 提示影像残存为无活性病变。选择合适的研究方法仍需要进一步探索。
放射治疗后CT和(或)MRI影像残存总是令人担忧, 多年以后仍有治疗失败的结果。McKelvie等[5]报道中位随访50(4~150)个月, 中位远处播散时间36(24~76)个月。Harada等[32]报道中位随访9(0.9~22)年, 6例对侧失败, 中位对侧失败时间84个月。本研究中位随访76.5(1~143)个月, 仅3例远处失败, 失败时间为放疗后21、42、45个月。远处播散时间与文献[5]一致, 对侧失败结果仍需进一步长期观察。
晶体遮挡技术的应用显著降低了白内障的发生[22, 27, 29]。Goda等[27]报道随访7年时晶体遮挡患者与未遮挡患者3级白内障发生率分别为15%和41%(P=0.003)。本研究中, 采用晶体减免技术与晶体未遮挡者3级白内障发生率13.6%(3/22)和42.9%(9/21)(P=0.045)。无遮挡病变的情况下, 应积极采用晶体减免照射技术减少白内障的发生。病变原发或累及眼睑者, 适宜采用眼屏蔽保护眼球的同时照射眼睑病变。
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|
| [32] |
|