


{kind=link}
{kind=link}
微创玻璃体切割术联合生物胶治疗原发性孔源性视网膜脱离的疗效和安全性
引用本文
王群, 赵杰, 侯宝杰. 微创玻璃体切割术联合生物胶治疗原发性孔源性视网膜脱离的疗效和安全性[J]. 武警医学, 2019,29(12): 1155-1158
WANG Qun, ZHAO Jie, HOU Baojie. Safety and effect of microincision vitrectomy with bio-glues for retinal holes sealing in rhegmatogenous retinal detachment[J]. Medical Journal of the Chinese People's Armed Police Forces, 2019,29(12): 1155-1158
Permissions
WANG Qun, ZHAO Jie, HOU Baojie. Safety and effect of microincision vitrectomy with bio-glues for retinal holes sealing in rhegmatogenous retinal detachment[J]. Medical Journal of the Chinese People's Armed Police Forces, 2019,29(12): 1155-1158
Copyright©2018, 《武警医学》编辑部
微创玻璃体切割术联合生物胶治疗原发性孔源性视网膜脱离的疗效和安全性
摘要
目的 探讨微创玻璃体切割术联合生物胶治疗原发性孔源性视网膜脱离的疗效和安全性。方法 选取2014-06至2017-06解放军总医院第三医学中心收治的原发性孔源性视网膜脱离患者21例,共21眼,微创玻璃体切割术(microincision vitrectomy surgeries, MIVS)联合应用生物胶来封闭视网膜裂孔,应用手术灌注液填充玻璃体腔。观察术中生物胶覆盖情况,以及术后视网膜复位成功率、矫正视力、眼压、炎性反应和并发症等情况。结果 术中生物胶与视网膜黏附良好,能成功封闭视网膜裂孔。通过间接检眼镜检查见生物胶膜在玻璃体切除术后(13.77±5.13)d已吸收。21例21只眼术中和术后视网膜复位成功,在随访期间视网膜脱离未复发。术后1年矫正视力0~2.15,平均(0.79±0.62),较术前矫正视力0~2.32,平均(0.93±0.74),显著提高。1例1只眼术后出现视网膜前膜,最终需要行前膜剥除术。2例2只眼术后7 d内出现一过性眼压升高,给予噻吗洛尔滴眼液治疗后眼压降至正常。出院随访期间未发现眼压异常情况。未发现明显的与生物胶相关的炎性反应或其他并发症。结论 MIVS中联合生物胶可成功封闭视网膜裂孔,促进孔源性脱离视网膜复位;眼内应用安全有效,可以作为MIVS联合气体填充的一种替代选择。
关键词:
生物胶; 孔源性视网膜脱离; 微创玻璃体切割术; 视网膜裂孔
中图分类号:R779.6
Safety and effect of microincision vitrectomy with bio-glues for retinal holes sealing in rhegmatogenous retinal detachment
Abstract
Objective To evaluate the safety and effect of microincision vitrectomy and bio-glue in sealing retinal holes for primary rhegmatogenous retinal detachment.Methods Between June 2014 and June 2017, 21 cases of primary rhegmatogenous retinal detachment patients (21 eyes) were selected from our Department of Ophthalmology. All the 21 patients were given microinvision vitrectomy, during which bio-glue was used to seal the retinal holes. At the end of surgery, a balanced saline solution was used to fill the vitreous cavity. The glue membrane, first-time retinal reattachment rate, corrected visual acuity, intraocular pressure and intraocular inflammatory reaction and complications were observed.Results The bio-glue could adhere fast to the retina during microincision vitrectomy. The bio-glue membrane was absorbed at (13.77±5.13)days postoperatively. All the retinal holes were totally sealed after surgery. The first-time retinal reattachment rate was 100%. At 12 months after microincision vitrectomy, the corrected visual acuity was significantly improved from 0-2.32,average(0.93±0.74),to 0-2.15,average(0.79±0.62). One eye was diagnosed with epiretinal membrane after vitrectomy and was finally given membrane peeling surgery. Two eyes in two cases developed an abnormal intraocular pressure at 7 days after vitrectomy. With the use of Timolol, the pressure returned to normal. During vitrectomy and 12 months of follow-up, there was no obvious inflammation or adverse effect.Conclusions The joint application of vitrectomy and bio-glue can seal retinal holes properly without the use of gas. It can be a new alternative to rehgmatogenous retinal detachment during microincision vitrectomy.
Keyword:
bio-glue; rehgmatogenous retinal detachment; microincision vitrectomy; retinal hole
孔源性视网膜脱离(rhegmatogenous reintal detachment, RRD)是眼科常见的致盲性疾病。目前临床治疗RRD最重要的是通过手术封闭视网膜裂孔, 达到解剖学视网膜复位, 这是RRD手术成功的标准[1, 2]。治疗RRD的主要手术方法是应用微创玻璃体切割术(microincision vitrectomy surgeries, MIVS); 但是MIVS需要依靠眼内空气、长效气体或者硅油等填充物的辅助作用, 禁止眼内液体再次进入视网膜下, 来完成视网膜复位; 对于下方视网膜裂孔导致的RRD成功率处于低限[3, 4, 5, 6, 7]。而眼内填充物的应用也可能引起许多并发症[8, 9]。因此, 如何能在保证视网膜成功复位的前提下, 减少相关并发症也已成为临床上RRD治疗的一个重要问题。近几十年, 生物胶在众多手术学科和内镜手术中的应用取得重大进展。大量临床研究成功应用生物胶止血、黏合组织和组织近似物; 生物胶在眼科手术中的应用也越来越广泛[10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20]。在目前的临床研究中, 生物胶的应用被认为是安全的[21]。本研究旨在探讨MIVS联合生物胶治疗原发性孔源性视网膜脱离的疗效和安全性。
1 对象与方法
1.1 对象
选取2014-06至2017-06我中心收治的原发性孔源性视网膜脱离患者21例, 手术21只眼。其中男9例, 女12例; 年龄22~68岁, 平均(49.4± 11.9)岁; 症状持续时间(20.6± 10.2)d; 视网膜裂孔1个12例, 2个及以上9例; 视网膜裂孔位置, 上方或中线11例, 下方8例, 上方和下方2例; PVR分级, A10例, B10例, C1 1例; 脱离累及黄斑4例; 高度近视11例。
下方六个钟点的视网膜脱离定义为下方视网膜脱离。排除标准:(1)病情诊断分级符合美国视网膜协会关于增生性玻璃体视网膜病变(proliferative vitreoretinopathy, PVR)分级标准的C2、C3级别; (2)非初次发病; (3)视网膜脱离范围大于3个象限; (4)有既往眼科手术史、有角膜混浊、有达到手术程度的白内障、存在其他内眼疾病史。本研究经我院伦理委员会批准开展, 患者均了解本研究的内容和目的, 并签署知情同意书。
1.2 材料
广州倍绣生物技术有限公司生产的倍绣医用生物胶套盒, 5.0 ml, 批准文号:国药准字S20110020。
1.3 手术方法
21例21眼行MIVS手术, 手术由同一主刀医师完成。术中行完全玻璃体后脱离后切除玻璃体, 周边玻璃体切除干净后液-气交换, 激光光凝视网膜裂孔和格子样视网膜变性区。根据生物胶使用说明提前准备好生物胶溶液。视网膜下液体吸除干净, 蛋白胶A 完全覆盖视网膜裂孔, 越过视网膜裂孔边缘约1 mm。 静置5 s后, 蛋白胶B覆盖于蛋白胶A的表面, 3 min后见视网膜裂孔表面形成半透明视网膜胶膜, 成功封闭视网膜裂孔。仔细检查周边视网膜。手术结束时, 灌注液填充玻璃体腔。
1.4 观察指标
一次手术成功率定义为初次手术后视网膜复位成功率, 并且在随访期间未发生视网膜脱离复发。记录分析矫正视力、眼压、眼内炎性反应和术后并发症等情况。
1.5 统计学处理
视力以 LogMAR进行统计分析, 根据文献[22]手动/眼前转换为LogMAR 2.28。使用SPSS 20进行统计分析, 以P< 0.05为差异有统计学意义。
2 结 果
2.1 手术情况
在MIVS术中, 生物胶成功覆盖在视网膜裂孔上形成胶膜。间接检眼镜检查生物胶膜在MIVS术后(13.77± 5.13)d完全吸收, B超检查生物胶膜不可见(图1)。生物胶成功封闭21例21眼视网膜裂孔, 21眼一次手术成功率为100%, 在随访12个月内未发生视网膜再次脱离或视网膜脱离复发(图2)。
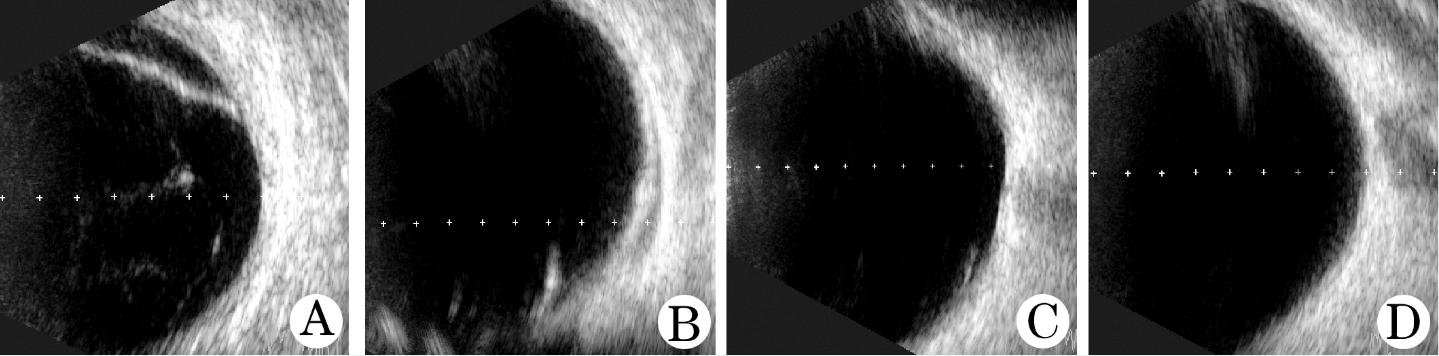 | 图1 MIVS联合生物胶治疗原发性孔源性视网膜脱离术前、术后超声图像 A.术前视网膜脱离; B.术后第1天见视网膜前胶膜较前吸收; C.术后第7天生物胶膜较前明显吸收; D.术后第13天生物胶膜完全吸收 |
 | 图2 MIVS联合生物胶治疗原发性孔源性视网膜脱离术前、术后眼底彩照 A.术前视网膜脱离; B.联合生物胶术后第1天, 见视网膜裂孔周围激光斑形成好, 视网膜裂孔表面见半透明状胶膜; C.MIVS联合生物胶术后第7天, 视网膜裂孔表面半透明胶膜明显较前吸收 |
2.2 矫正视力
术前矫正视力Log MAR为0~2.32, 平均(0.93± 0.74); 术后12个月BCVA为0~2.15, 平均(0.79± 0.62); 术前和术后12个月BCVA比较, 差异有统计学意义(P=0.008)。其中10眼术后视力提高超过2行, 7眼视力无变化。4眼视力下降, 其中3眼下降1行, 1眼下降3行。
2.3 眼内压
术前21眼眼内压为(13.50± 3.21)mmHg。随访12个月, 19眼眼内压正常。在MIVS后7 d内, 2眼眼内压一过性升高, 眼内压最高不超过30 mmHg, 给予噻吗洛尔滴眼液后眼内压降至正常, 局部治疗7 d停药后眼内压持续正常。
2.4 黄斑前膜形成
1眼在MIVS术后3个月诊断为黄斑前膜, 行黄斑前膜剥除手术。
2.5 安全性
21眼21例中未发现其他眼部检查可见的变化。随访12个月未发现明显的眼内炎性反应或全身性不良事件。
3 讨 论
RRD的手术方式主要是MIVS和巩膜外垫压。两种手术治疗目的都是复位视网膜, 通过激光或冷冻在视网膜裂孔周围产生牢固坚实的脉络膜视网膜间粘连, 由蛋白质凝固产生的脉络膜视网膜粘连在孔周进行激光后的前3 d粘连力量较弱, 在光凝后约第5天开始逐步由粘连力较强的炎性瘢痕替代[23]。手术成功的另一个关键是在牢固坚实的脉络膜视网膜粘连形成之前要预防玻璃体腔内液体再次通过视网膜裂孔进入到视网膜下腔。MIVS手术需依赖眼内填充物如长效气体或硅油来成功复位视网膜。长效气体或硅油等眼内填充物能够在跨视网膜裂孔区域保持足够大的表面张力来阻止液体进入视网膜裂孔, 从而保持视网膜裂孔周围干燥无水, 并产生一定的加固脉络膜视网膜粘连的作用力[24, 25]。MIVS联合眼内填充物的应用是目前治疗RRD的主要手术方式。但眼内填充物并不安全, 研究发现长效气体填充或硅油充填会引起许多并发症, 如继发性青光眼、白内障、增生性玻璃体视网膜病变和带状角膜变性等[26, 27]。此外, 眼内气体填充时气体的表面张力可能为视网膜前膜的形成提供一定的支架作用, 视网膜裂孔的位置对于MIVS手术的成功率也有重要影响, 通常下方视网膜裂孔引起的视网膜脱离需要高浓度的长效气体或应用重硅油填充来复位视网膜, 这样更容易引起填充并发症[28, 29]。
目前, 临床上生物胶主要作为止血剂应用, 可快速有效地促进密封或黏合组织, 并有助于止血、促进伤口愈合, 且不引起明显的炎性反应和异物排斥反应。本研究将生物胶作为玻璃体腔填充物的替代选择, 因为生物蛋白胶的应用可以在牢固的脉络膜视网膜粘连形成前, 通过生物胶膜阻止玻璃体腔内液体再次通过视网膜裂孔进入视网膜下腔造成视网膜脱离。本研究中, 随访期间所有21只眼视网膜均一次性成功复位, 高于文献[4, 5, 6, 7]报道的成功率。
生物胶能较好地黏附于视网膜形成胶膜, 阻止液体进入视网膜下的同时可隔绝视网膜色素上皮细胞和炎性因子通过视网膜裂孔渗漏进入玻璃体腔, 我们认为一定程度上有利于降低术后视网膜增殖的产生和前膜的形成。视网膜前膜是RRD的MIVS手术常见并发症, 发生率为4.4%~12.8%[30, 31]。本研究中, 1眼(4.76%)在术后形成黄斑前膜。生物胶并未增高视网膜前膜的发生率, 由于本研究的样本量有限, 不能明确该眼的视网膜前膜形成是否与生物胶的应用有关。
在体评估安全性和炎性反应对于任何生物材料的临床应用都至关重要。我们既往的基础研究未发现兔眼内应用生物胶会导致兔眼明显的炎性反应和视网膜毒性。该生物胶已在我国普外科、心胸外科、妇产科、骨科、神经外科和泌尿外科等学科被广泛应用, 可用于止血、封闭(黏合)伤口、促进伤口愈合及预防组织粘连, 并可作为药物缓释载体。
总之, 本研究采用MIVS手术联合生物胶的应用能成功封闭视网膜裂孔, 促进RRD视网膜复位, 生物胶可作为MIVS联合眼内填充物的另一种选择, 能显著降低眼内填充物应用的并发症发生率, 临床应用安全可靠。
The authors have declared that no competing interests exist.
参考文献
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|